Indentify the following:
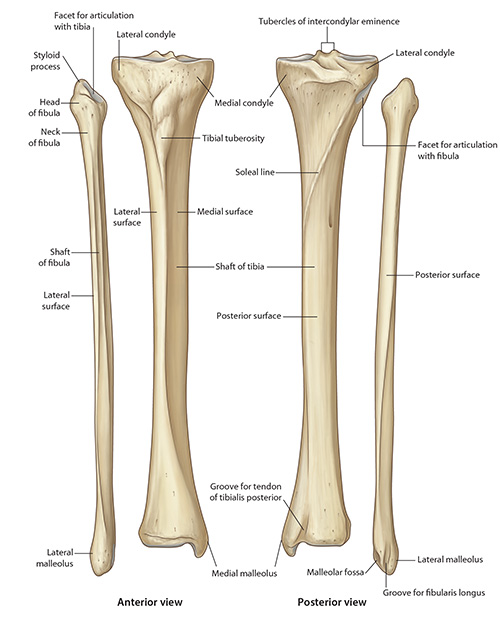
The Head of the Fibula - The head of the fibula is the expanded proximal end. It has the shape of an irregular cuboid. Its anterior, lateral and posterior aspects are palpable. Projecting proximally from its postero-lateral aspect is a conical process called the styloid process. Attached to the styloid process is the arcuate ligament.
The Styloid Process of the Fibula - The styloid process of the fibula is a conical, upward projection of bone on the postero-lateral aspect of the fibular head. It is sometimes palpable. The arcuate ligament is attached to it.
The Neck of the Fibula - The neck of the fibula is the constriction which marks the junction between the head and shaft of fibula. It is thinly wrapped in muscle; fibularis longus laterally, extensor digitorum longus anteriorly and soleus posteriorly. A very important and close topographical relation is the common fibular nerve as it winds around the lateral aspect of the fibular neck.
The Shaft of the Fibula - The shaft of the fibula presents a fairly generous surface on its lateral aspect called the peroneal surface. Fibularis longus arises from the upper two-thirds while fibularis brevis arises from the lower two-thirds, of this surface. The peroneal surface of the fibula is limited by anterior and posterior borders. Medial to the anterior border of the fibula and very close to it is the interosseous border of the fibula. Between the anterior border and interosseous border, is the rather narrow extensor surface of the fibula. Extensor digitorum longus arises from the upper three-fourths of this surface while fibularis tertius arises from the lower quarter of this surface.
The Lower End of the Fibula - The lower end of the fibula, also called the lateral malleolus, presents a subcutaneous and easily palpable lateral surface. The medial surface of the lower end of the fibula has a smooth triangular facet which articulates with a reciprocal facet on the lateral aspect of the body of the talus, this being part of the talocrural articulation. Posterior to the triangular articular facet is a fossa termed the malleolar fossa. This gives attachment to ligaments which contribute to the stability of the talocrural articulation.
The Superior Tibio-Fibular Joint - The superior tibio-fibular joint may be dislocated traumatically and in this case, the fibular nerve may be vulnerable. Clicking and recurrent subluxation of this joint may occur following the initial trauma. The resultant pain may be helped by local injection of anesthetic plus hydrocortisone.