
Lab2 - Module 2 - Anatomy of the Scapular Region: Page 7 of 7
CASE REPORT CONCLUSION:Based on the examination and the most likely diagnosis would be a rotator cuff tear. The most likely muscle involved would be the supraspinatus. Remember the supraspinatus initiates the first 10 – 15 degrees of glenohumeral joint abduction. Additionally, the patient exhibited a positive empty can test which is indicative of a supraspinatus tear. |
|
The patient was unable to lift their arm over their head. That could be due to the weakened state of the supraspinatus so the deltoid never gets into a position to take over. Or it could be because of pain from the torn tendon hitting the acromion process or coracoacromial ligament. |
|
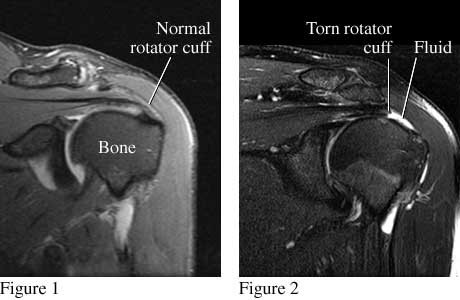
There are many things that could also cause similar symptoms. One way to differentiate is with a MRI. |
 |
DIFFERENTIAL DIAGNOSIS: |
|
|